Juvenile Idiopathic Arthritis
Overview:
Not a specific disease, term to identify all forms of idopathic arthritis that begin before age 16 and persists for more than 6 wks.
Common Signs
The classic signs of JIA are articular effusion and synovial hypertrophy. Children will often complain of joint and muscle pain, joint
stiffness in the morning and after prolonged rest, night pain, and tenderness to palpation. Due to chronic inflammation, secondary problems develop,
including decreased ROM, decreased strength, joint deformities, ligamentous laxity, joint subluxation, growth retardation, and osteoporosis
Categories According to International League of Association for Rheumatism
Systemic-onset JIA/Still's Disease
Polyarticular JIA
Oligoarticular/Pauciarticular JIA 50% of all cases
Psoriatic JIA
Enthesitis-related JIA
Causes:
Autoimmune disease. Etiology unknown, but may be connected to genetic disease in combination with environmental triggers.
Risk Factors:
Variants in Human Luekocyte Antigens HLA, Formula feeding vs. breastfeeding, Infection, Maternal smoking
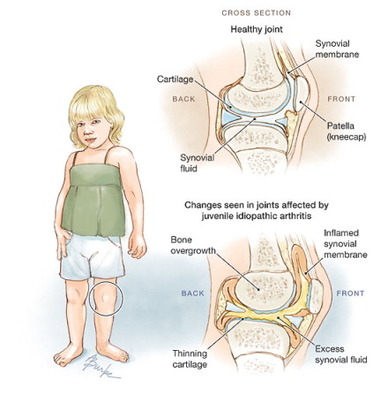
Pathogenesis:
Autoimmune response causes synovitis, inflammation of the synovial tissue surrounding the joints and tendons. Leads to synovial hypertrophy that results in formation of pannus that covers articular surface and causes damage to cartilage. Also leads to fibrosis and contractures of the surrounding tissue.
Contraindications/Precautions:
During acute flare up avoid over-activity such as agressive stretching and strengthening. Rest, gentle ROM and strengthening in pain-free range are recommended. A child with Systemic JIA may have medical restriction to be aware of. Also, good to be aware of joint instability and subluxation.
Examination:
History:
A family history of rheumatological conditions
Precipitating factors: trauma, recent illness, medication charnge, activity change
Unexplained weight loss
Frequency of flare ups at the involved joints
Medications:
NSAIDs, corticosteriod injections, methotrexate, biological agents to affect cytokines in disease process
Recurrent Illnesses
Diagnostic Tests/Imaging
Clinical evaluation is the main tool utilized in diagnosing JIA; however, X-rays, magnetic resonance imaging (MRI), ultrasonography, computed tomography (CT), and laboratory tests may aid in the diagnosis. No laboratory test can diagnose JIA. Laboratory tests will screen for anemia, increased white blood cell count, elevated erythrocyte sedimentation rate (ESR), positive rheumatoid factor, and positive antinuclear antibody test
Tests and Measures
Gait/locomotion
Complete a gait assessment as indicated and appropriate. It has been noted that children with JIA have a decreased velocity, cadence, and stride length. Additional common deviations include increased anterior pelvic tilt with decreased hip extension and ankle plantar flexion at terminal stance.
ROM
Muscle contractures will typically develop in the flexors. ROM limitations in the hip include decreased hip extension, abduction, and internal rotation. Typical limitations in the knee include decreased extension. In the UE, pay particular attention to the elbow, wrist, and hand. Assess LE flexibility, paying special attention to the hamstrings, iliopsoas, adductors, and iliotibial band.
Sensory
Clinician may want to assess proprioception, kinesthesia, and ight touch as they may be altered by degree of swelling
Joint integrity and mobility
Swelling around the hip is difficult to detect unless the child is thin.
Note joint end feels
The hip is rarely the primary joint involved at onset of JIA, but may become involved early, particularly in systemic JIA
Half of patients with systemic JIA develop clinical hip disease
Muscle Strength
Typically, weakness will be present in the extensors. Note muscle atrophy and assess thigh/calf girth for symmetry. Note compensatory movements during developmental activities or during functional tasks.
Assessment/Outcome Measures:
Functional mobility
Clinicians may use the Pediatric Evaluation of Disability Inventory (PEDI) tool or the wee-FIM to evaluate functional skills. Note proficiency, movement
quality, endurance, and speed when performing functional tasks..
Additional Outcome Measures:
Pediatric Quality of Life Inventory (PedsQL)
Rheumatology Module 3.0
Juvenile Arthritis Quality of Life Questionnaire (JAQQ)
Pediatric Rheumatology Quality of Life Scale (PRQL),
Childhood Arthritis Health Profile (CAHP)
Juvenile Arthritis Multidimensional Assessment Report (JAMAR)
See Juvenile Idiopathic Arthritis References
Not a specific disease, term to identify all forms of idopathic arthritis that begin before age 16 and persists for more than 6 wks.
Common Signs
The classic signs of JIA are articular effusion and synovial hypertrophy. Children will often complain of joint and muscle pain, joint
stiffness in the morning and after prolonged rest, night pain, and tenderness to palpation. Due to chronic inflammation, secondary problems develop,
including decreased ROM, decreased strength, joint deformities, ligamentous laxity, joint subluxation, growth retardation, and osteoporosis
Categories According to International League of Association for Rheumatism
Systemic-onset JIA/Still's Disease
Polyarticular JIA
Oligoarticular/Pauciarticular JIA 50% of all cases
Psoriatic JIA
Enthesitis-related JIA
Causes:
Autoimmune disease. Etiology unknown, but may be connected to genetic disease in combination with environmental triggers.
Risk Factors:
Variants in Human Luekocyte Antigens HLA, Formula feeding vs. breastfeeding, Infection, Maternal smoking
Pathogenesis:
Autoimmune response causes synovitis, inflammation of the synovial tissue surrounding the joints and tendons. Leads to synovial hypertrophy that results in formation of pannus that covers articular surface and causes damage to cartilage. Also leads to fibrosis and contractures of the surrounding tissue.
Contraindications/Precautions:
During acute flare up avoid over-activity such as agressive stretching and strengthening. Rest, gentle ROM and strengthening in pain-free range are recommended. A child with Systemic JIA may have medical restriction to be aware of. Also, good to be aware of joint instability and subluxation.
Examination:
History:
A family history of rheumatological conditions
Precipitating factors: trauma, recent illness, medication charnge, activity change
Unexplained weight loss
Frequency of flare ups at the involved joints
Medications:
NSAIDs, corticosteriod injections, methotrexate, biological agents to affect cytokines in disease process
Recurrent Illnesses
Diagnostic Tests/Imaging
Clinical evaluation is the main tool utilized in diagnosing JIA; however, X-rays, magnetic resonance imaging (MRI), ultrasonography, computed tomography (CT), and laboratory tests may aid in the diagnosis. No laboratory test can diagnose JIA. Laboratory tests will screen for anemia, increased white blood cell count, elevated erythrocyte sedimentation rate (ESR), positive rheumatoid factor, and positive antinuclear antibody test
Tests and Measures
Gait/locomotion
Complete a gait assessment as indicated and appropriate. It has been noted that children with JIA have a decreased velocity, cadence, and stride length. Additional common deviations include increased anterior pelvic tilt with decreased hip extension and ankle plantar flexion at terminal stance.
ROM
Muscle contractures will typically develop in the flexors. ROM limitations in the hip include decreased hip extension, abduction, and internal rotation. Typical limitations in the knee include decreased extension. In the UE, pay particular attention to the elbow, wrist, and hand. Assess LE flexibility, paying special attention to the hamstrings, iliopsoas, adductors, and iliotibial band.
Sensory
Clinician may want to assess proprioception, kinesthesia, and ight touch as they may be altered by degree of swelling
Joint integrity and mobility
Swelling around the hip is difficult to detect unless the child is thin.
Note joint end feels
The hip is rarely the primary joint involved at onset of JIA, but may become involved early, particularly in systemic JIA
Half of patients with systemic JIA develop clinical hip disease
Muscle Strength
Typically, weakness will be present in the extensors. Note muscle atrophy and assess thigh/calf girth for symmetry. Note compensatory movements during developmental activities or during functional tasks.
Assessment/Outcome Measures:
Functional mobility
Clinicians may use the Pediatric Evaluation of Disability Inventory (PEDI) tool or the wee-FIM to evaluate functional skills. Note proficiency, movement
quality, endurance, and speed when performing functional tasks..
Additional Outcome Measures:
Pediatric Quality of Life Inventory (PedsQL)
Rheumatology Module 3.0
Juvenile Arthritis Quality of Life Questionnaire (JAQQ)
Pediatric Rheumatology Quality of Life Scale (PRQL),
Childhood Arthritis Health Profile (CAHP)
Juvenile Arthritis Multidimensional Assessment Report (JAMAR)
See Juvenile Idiopathic Arthritis References
