Hip Labral Tears
Overview:
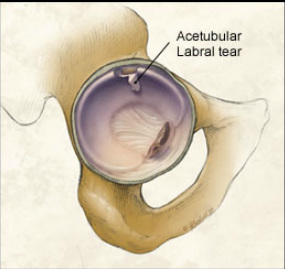
The hip joint consists of a ball and socket joint which is surrounded by a dense layer of tissue. The labrum, or acetabular labrum, is made up of a fibrocartilaginous structure which outlines the socket of this joint. The function of the labrum is to serve as a shock absorber, joint lubricator, and pressure distributor. It also resists lateral and vertical motion of the femoral head and helps to stabilizes the femoral head by deepening the socket in which it lies.1
Pathogenesis: Tearing of the labrum found within the hip joint. This can lead to reduced stability of the femoral head and my predispose one to degenerative wear and tear chondral lesions, even more so with those that have structural abnormalities of the hip.
Causes/Risk Factors:
Acetabular labral tears may occur during a sporting activity or other instances where there was a hip injury from traumatic twisting, planting, or cutting.2
People that have underlying abnormal hip morphology, are exposed to high impact activities, or participate in sports that involve high force twisting and extreme pivoting positions of the hip may be at risk
Clinical Presentation:
People who have these tears may complain of hip or groin pain or report the sensation of catching or locking of the hip throughout the hip range of motion.2
During the physical examination patients may experience pain with hip flexion to 90 degrees, adduction and internal rotation. Labral tears may be diagnosed in both sexes and throughout all ages, ad studies have reported that symptomatic labral tears occur more frequently in women than in men.1 Special tests that can be used to help with the diagnosis of a labral tear include the FABER and FADIR tests.
Contraindications/Precautions:
Physical Therapists who treat people with labral tears should have a fall prevention protocol if treating in inpatient setting. Outpatient settings shouls also take measures to prevent falls while exercising, especially during gait, balance, and other functional training. Following surgery the patient should not perform: 3
Straight leg raises
Sit-ups
Hip extension past neutral
Cycling on recumbent bike
Differential Diagnosis:
Labral tears are associated with slipped capital epiphyses, Legg-Calve-Perthes disease, dysplasia, and capsular laxity/hypermobility, and may contribute to femoroacetabular impingement1
Outcome Measures:
Some of the most common outcome measures that are used for rehab after a labral tear are:
Clinical Bottom Line:
If a hip labral tear is suspected, the patient should be referred back to their primary physician for further test to see if surgery or other medical interventions are needed to correct the impairment. Conservative therapy may also be used for treatment, or a proper physical therapy program may be applied after surgical correction.
See Hip Labral Tear References:
The hip joint consists of a ball and socket joint which is surrounded by a dense layer of tissue. The labrum, or acetabular labrum, is made up of a fibrocartilaginous structure which outlines the socket of this joint. The function of the labrum is to serve as a shock absorber, joint lubricator, and pressure distributor. It also resists lateral and vertical motion of the femoral head and helps to stabilizes the femoral head by deepening the socket in which it lies.1
Pathogenesis: Tearing of the labrum found within the hip joint. This can lead to reduced stability of the femoral head and my predispose one to degenerative wear and tear chondral lesions, even more so with those that have structural abnormalities of the hip.
Causes/Risk Factors:
Acetabular labral tears may occur during a sporting activity or other instances where there was a hip injury from traumatic twisting, planting, or cutting.2
People that have underlying abnormal hip morphology, are exposed to high impact activities, or participate in sports that involve high force twisting and extreme pivoting positions of the hip may be at risk
Clinical Presentation:
People who have these tears may complain of hip or groin pain or report the sensation of catching or locking of the hip throughout the hip range of motion.2
During the physical examination patients may experience pain with hip flexion to 90 degrees, adduction and internal rotation. Labral tears may be diagnosed in both sexes and throughout all ages, ad studies have reported that symptomatic labral tears occur more frequently in women than in men.1 Special tests that can be used to help with the diagnosis of a labral tear include the FABER and FADIR tests.
Contraindications/Precautions:
Physical Therapists who treat people with labral tears should have a fall prevention protocol if treating in inpatient setting. Outpatient settings shouls also take measures to prevent falls while exercising, especially during gait, balance, and other functional training. Following surgery the patient should not perform: 3
Straight leg raises
Sit-ups
Hip extension past neutral
Cycling on recumbent bike
Differential Diagnosis:
Labral tears are associated with slipped capital epiphyses, Legg-Calve-Perthes disease, dysplasia, and capsular laxity/hypermobility, and may contribute to femoroacetabular impingement1
Outcome Measures:
Some of the most common outcome measures that are used for rehab after a labral tear are:
- VAS
- Goniometry
- MMT
- Berg Balance Scale
- FIM, TUG test
Clinical Bottom Line:
If a hip labral tear is suspected, the patient should be referred back to their primary physician for further test to see if surgery or other medical interventions are needed to correct the impairment. Conservative therapy may also be used for treatment, or a proper physical therapy program may be applied after surgical correction.
See Hip Labral Tear References:
